
For Appointments Call 03 6326 6999
Journey towards centralization and recovery.

Lumbar Radicular Pain/Radiculopathy. Centralization of symptoms. Changing symptomatic disc to asymptomatic disc.
Lumbar radicular pain with or without radiculopathy is one of the most common complaints evaluated by spinal surgeons. Its prevalence has been estimated to be 3-5% of the population, affecting both men and women. In addition to lifestyle factors and previous trauma, age is a primary risk factor. Symptoms typically begin in the middle of the patients life, with men often affected in their 40s while women are affected in their 50s and 60s [1–2]. Underlying pathologies, involving the spinal canal, thecal sac, foramine, laeral recess either irritate or compress the exciting nerve root of the patient. These pathologies include, but are not limited too, spondyloarthropathies, disc herniation, canal stenosis, facet degenerations, ligamentous hypertrophies, tumors, infection, inflammation, tuberculosis and other space occupying lesions.
Treatment Options:
The need for surgical intervention has been extensively studied, yet controversy exists. According to an international survey, surgeons around the world indicated one of the assumptions for an operative intervention is the failure of rehab. and conservative Rx.
Therefore, a cost effective, evidence-based approach with promising outcomes, is Physical therapy which focuses on Centralization of symptoms followed by functional based rehab.
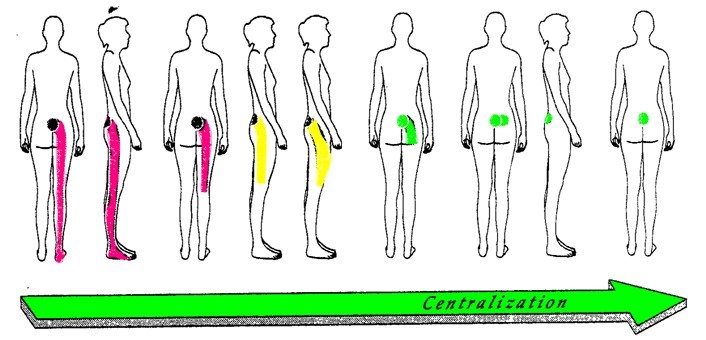
The aim of this stage is to centralize the symptoms. This can be achieved by Mackenzie Extension exercises, but some cases respond better with flexion programs: This program was introduced by Robin McKenzie a New Zealand physical therapist. Many studies have confirmed the reliability and cost effectiveness of McKenzie type of spinal exercises.